Patch testing is part of the diagnostic pathway for people who have rashes.
Patient info
People in the community may not be very familiar with patch testing and how it works and why it is used.
Patch testing is a very specialised test, performed primarily by dermatologists in specialised centres. It is often needed when a person’s rash will not heal or get better or keeps recurring, despite treatment.
Why have you been referred for patch testing? Patch testing is often used when a rash will not heal, will not get better, or keeps recurring despite treatment.

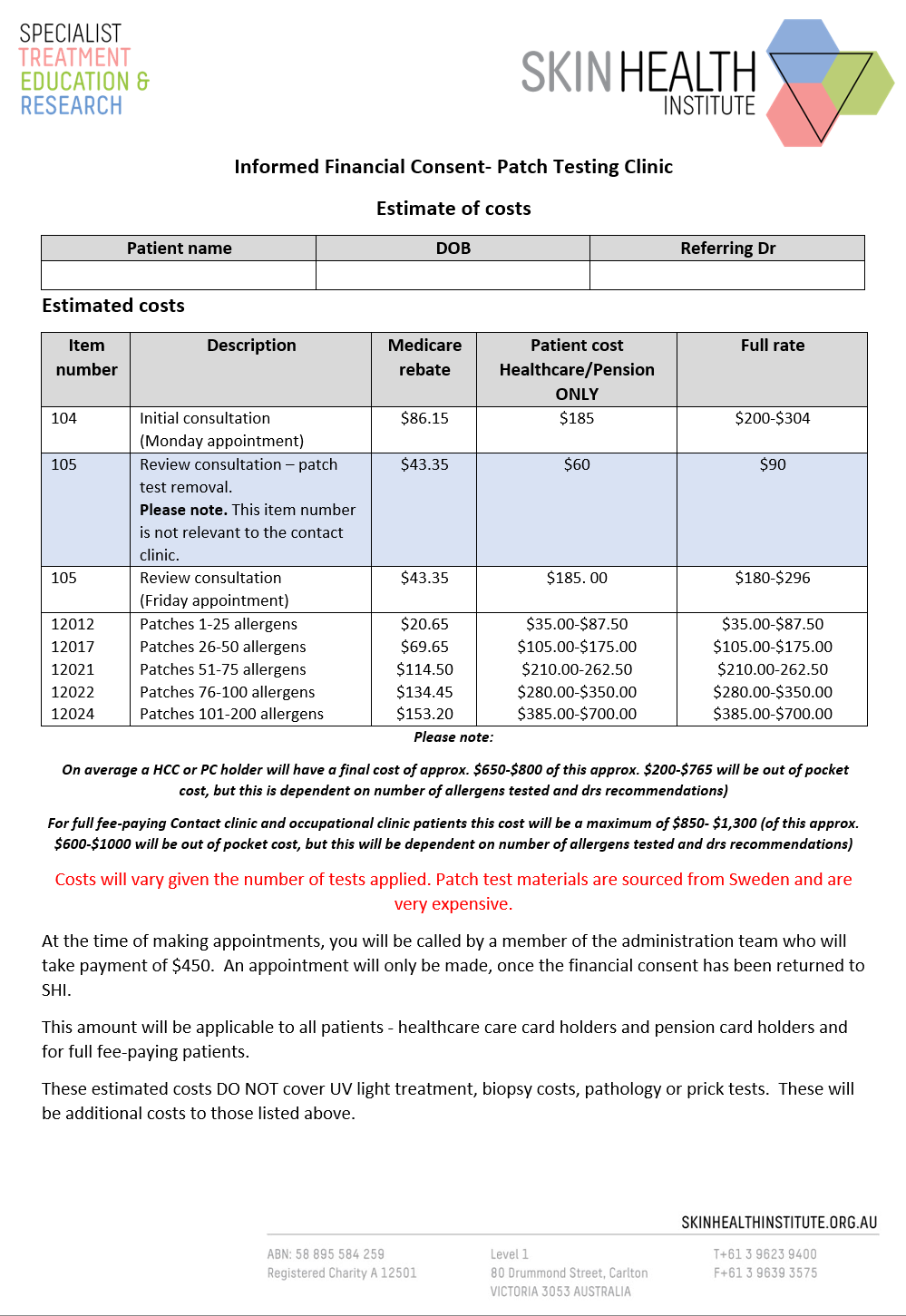
Patch testing costs
Patch testing is expensive.
Along with the three appointments needed to fulfil the patch testing process, the purchase of allergens from Sweden and America adds to the cost of this form of testing. There are only two places in the world that manufacture these allergens, hence they are costly. The team also requires very specialised knowledge and upskilling is often needed.
The costs are listed in the financial consent below. All patients are sent this consent form and it must be returned along with the $450 deposit prior to appointments being made.
What to know before attending patch testing
There is often confusion about whether a person can or cannot be tested on certain medications and biologic drugs. Some medications can reduce the size of patch test reactions or sometimes stop reactions occurring entirely, meaning the patch test results cannot always be reliable.
Research indicates that patch testing can be done in most situations, but if possible, testing before starting a biologic drug is recommended, or have the biggest gap possible between injection and patch testing. When patch testing on upacitinib (Rinvoq), stop on the Friday before testing if patch testing starts on the Monday. There is not a lot of data available on these drugs and how they impact patch testing results. We know some drugs diminish or reduce the strength of the reactions, possibly leading to false negative reactions.
Oral corticosteroids should ideally be ceased at least 48 hours before testing. On rare occasions, those with severe dermatitis or eczema may have to continue on a small dose (5-10mg maximum) to ensure the skin is maintained at a level where patch testing is possible. The dermatologist conducting the patch testing should be aware that the patient is taking oral steroids. This should also be noted when reactions are being read as the strength of reactions may be reduced.
Medications such as methotrexate, azathioprine and cyclosporine may be continued during the patch testing process, as long as the dermatologist is aware of this.
Other medications such as antibiotics can also be taken during the patch testing process, as they do not impact on patch testing results.
Medication and skin considerations
Topical Corticosteroids
Topical corticosteroids may be continued, except on the back during the period of testing. If applying on an area where patches are to be applied, topical steroid use should be ceased 3-7 days beforehand. If ceased closer to the period of testing, be mindful of false negative reactions.
Antihistamines
Antihistamines may be used as they will not affect test results. However, they can impact prick testing results.
Rashy skin/eczema
Patch testing on rashy or eczematous skin is generally discouraged, as patch testing on such skin can cause a flare up, therefore making reading of results difficult.
We would recommend avoiding applying patches on areas of skin that have an active rash and to consider patch testing once the skin has improved.
Occasionally a patient with severe eczema or dermatitis will be patch tested whilst on a low dose of oral corticosteroids, particularly if there is a risk that skin will deteriorate if they are stopped. However, be aware that reactions may be lessened as a result.
Be cautious when applying patches to skin with recent eczema or very dry skin. Some patches can stick too firmly and be difficult to remove.
Pregnancy and breast feeding
At SHI, we avoid patch testing in the first trimester of pregnancy, because the side effects of patch testing on the baby are unknown.
Patch testing is considered safe in the 3rd trimester, if absolutely necessary. Otherwise wait until the baby is born.
On the other hand, some believe that patch testing in pregnancy should not be performed despite a lack of evidence suggesting that allergens used during testing could pass through to the foetus.
Patch testing a breastfeeding mother is considered to be safe.
Please call us, if you find out you are pregnant whilst waiting to attend your patch test appointments, as they may need to be rescheduled.
Sun exposure and UV light treatment
There should be no sun exposure or phototherapy to the back for a minimum of 7 days prior to testing. Theoretically sunlight exposure before testing may reduce the immune response of the skin and therefore affect the test results, although clear-cut evidence is lacking. A patient should not attend patch testing with sunburn. Please call us if you are sunburnt close to your appointment date, as testing may need to be rescheduled.
Practical information during testing
What does patch testing look like?
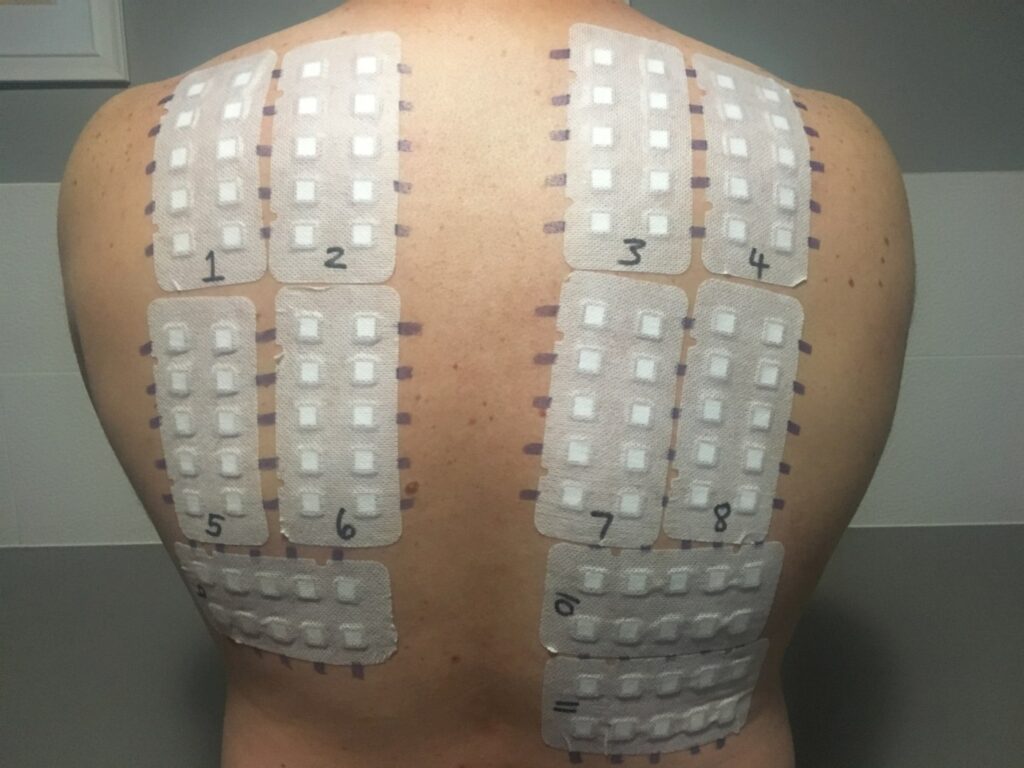
The patches are like big stickers that applied to the back. These are applied on a Monday and removed on a Wednesday, with final reading of results on the Friday.
Where are patches applied
The patches are normally applied to the back and occasionally the arms.
What clothes to wear during testing
Loose clothing that is dark in colour is best. On occasion, some of the coloured allergens can leak through the patch, hence dark clothing will prevent staining.
Exercise during testing
Light walking is permitted but strenuous sweaty activity and gym work is discouraged, as the patches can loosen and fall off.
Can I still work?
Work is permitted, but if strenuous work, with large arm movements is required, work modification or time off may be needed. Some people working in some occupational groups may require time off for approx. 2 days whilst patches are in place.
What if my patches become loose?
If patches start to loosen or peel off on the corners, Micropore tape can be applied. The patches used generally stick quite firmly but on occasion can peel, especially if there is lots of sweating and physical activity.
What if they get really itchy or sore?
It is very rare for patches to become sore and painful during patch testing. But if the patches do become very uncomfortable, please call the phone number on your information sheet.
There are some recommendations that you can try to settle itchiness during testing:
- Antihistamines can be used if very itchy.
- A cold ice pack wrapped in a tea towel or cloth and held against the itchy patches can be useful in reducing itch.
- Leaning up against something cold like a fridge door or cold glass window can also be beneficial.
- Patches should not cause nausea or headaches.
- People can feel sweaty, hot and stinging just after patches are applied but this should settle quickly.
Questions about allergy and patch testing
People are not born allergic to substances, but they can develop contact allergies during their life.
Why have I developed my allergy now, when I have been using this product for years?
People are not born allergic to substances, but they can develop contact allergies during their life. To become allergic to something, you must have been exposed to it before. Whilst it is possible that someone can develop allergic contact dermatitis to something after only using it once, there is often a long history of exposure to or use of a substance before a person becomes allergic to it. The exact reasons that some people develop allergy, whilst others do not, are poorly understood. The timing of allergy developing is also often unclear.
How long will I be allergic to this substance?
Unfortunately, the type of allergy that causes allergic contact dermatitis lasts for life. You will therefore have to continue to avoid exposure to the problem substance for the rest of your life. Your body has learnt to react to this substance and each time that you are exposed to it, it will produce an allergic reaction, likely resulting in a skin rash.
Can it be treated?
The rash that develops can be treated, but there is no cure or treatment that will stop you being allergic to a substance. The best treatment is to avoid exposure to the substance in the future. By contrast, some allergens that cause immediate reactions, such as grass, mould and trees causing hay fever and asthma, can be treated with desensitisation. This is performed by allergists and is not available in our clinic.
Will I develop more allergies?
There is always the chance that you will develop allergies to other substances in the future. This might happen to substances that you have been tested to before and were not allergic to at that time. This does mean that a negative patch test now does not mean that you will not become allergic to a substance in the future.
Apart from patch testing, is there any other way to diagnose contact dermatitis?
Unfortunately, there is not. Patch testing has been used for over 100 years to investigate the causes of allergic contact dermatitis. There have been advances with the technology that is used, but the basic process has remained the same. Other types of allergy such as contact urticaria can be investigated in different ways, for example by skin prick testing and special blood tests. These are often performed alongside patch testing if the patient’s story suggests that there is more than one type of allergy present. Prick testing is often used to diagnose food allergies or allergies to grass and pollen.
Is this all I am allergic to?
We can only diagnose allergy by testing you to a substance. Over 5,000 substances have been reported to cause allergic contact dermatitis, so it is not possible to test you to all of these.
We therefore interview each patient carefully to help decide what the most likely problem substances are, and test these. If you or we do not suspect a particular substance, then we might not test it, and this allergy would remain unknown.
How long will it take my skin to get better?
This is a difficult question. If the particular substance can be avoided, then the rash should settle within a few weeks. This will take longer if there is continued exposure, or if the initial rash was very severe, or had been there for a long time.
It is important to use the treatments for the rash that your doctor or dermatologist has suggested, until the rash has resolved. The skin will remain quite easily irritated for some time after it appears to be better, so good skin care is essential.
Sometimes additional treatments may be required. These include ultra-violet light treatment or Grenz ray treatment. Patients are normally referred back to their referring doctors for such treatments. In addition, sometimes oral (tablet) medications may be necessary for a while, to calm rashes down.
What if my skin does not get better?
There may be many reasons why your skin does not get better:
- There might be continuing exposure which you are not aware of to a substance that you are allergic to.
- If the initial rash was very severe, it can sometimes take many weeks to resolve.
- It is possible that you are allergic to other substances that were not tested for during patch testing. You may still be exposed to these, and these may be stopping your skin from returning to normal.
- Because your skin can be easily irritated, even frequent hand washing and ‘wet work’ may be a problem.
All of my patch tests are negative, what does this mean?
There are two main types of contact dermatitis. Allergic contact dermatitis is diagnosed by patch testing. Whilst irritant contact dermatitis is the most common type of dermatitis, there is no specific test for it. So, doctors test for allergy and if the tests are negative, then this points to irritation. However, there are several other skin conditions which could be the cause of the problem, and the dermatologist will discuss these with you.
What to do after patch testing
Getting marks off my back
The purple lines on your back will gradually wear off in time, once you return to showering normally. Alcohol swabs can also remove the purple lines.
It is best if the lines remain visible, if possible, for 10 days after your last patch testing appointment, in case there are any late reactions.
Can I have a reaction after my last appointment?
Yes, it is possible. Some allergens are late reactors such as corticosteroids and some metals. Checking your back for up to 10 days can be important. If you suspect you have had a late reaction, please take a photo and email to the [email protected].
Please refer to the information sheet about taking photos of late reactions. Insert link here.
How long do reactions last?
Reactions can remain visible on the back for a few weeks after the last appointment. But on occasion they can last up to a month if the reactions are strong. Using topical corticosteroids can help with healing these reactions.
What if patch tests are negative?
Some people are often disappointed that their patch testing is negative. But it should be considered a good thing, as sometimes avoiding allergens can be tricky. Patch testing is often used to exclude allergy as a cause of the skin rash, meaning once excluded other diagnoses may be considered and treatments can be considered.
Late reactions
Checking your back for up to 10 days can be important because some allergens are late reactors.
If you suspect a late reaction, please take a photo and email it to [email protected].
Replace with supporting image
Contact Dermatitis
What is contact dermatitis?
Contact dermatitis is a skin condition, which appears similar to eczema. Sometimes people use the words ‘eczema’ and ‘dermatitis’ to mean the same thing, but they are different. Contact dermatitis is an inflammatory skin condition caused by external substances touching the skin. Occupational contact dermatitis means that the dermatitis is caused by something you are contacting at work.
Contact dermatitis usually affects the hands, because it is the hands that are most commonly touching substances or products, especially at work. But it can also affect the arms, face or legs, in fact any part of the body.
Skin dryness is usually the first sign of dermatitis and often starts in the web spaces between the fingers.
Dermatitis can make the skin:
- Dry
- Itchy
- Red
- Split and crack
- Flake and peel
- Burn and sting
- Develop small blisters
Like eczema, contact dermatitis can be very distressing and unsightly, and people often find the appearance of their skin embarrassing. It can interfere with sleeping, especially when it is very itchy. In some circumstances, dermatitis can become so severe that some people have to take some time off work or in severe cases, give up their job or career altogether. However, it can often be managed with appropriate treatment and good skin care.
When dermatitis develops the skin may take months to heal, even once it looks like it has returned to normal.

Dermatitis can often impact people working in certain occupations as well, especially those who contact lots of irritating substances or perform irritating tasks such as hand washing or wet work or have frequent contact with allergens. These occupations can include:
- Hairdressing
- Healthcare
- Food handling
- Manufacturing
- Construction
- Printing
- Metal working
- Automotive industry

There are 3 main types of dermatitis
Irritant contact dermatitis
The most common type of contact dermatitis.
Allergic contact dermatitis
A delayed type of allergy.
Contact urticaria
This includes latex allergy, which is a type of contact urticaria.
Irritant Contact Dermatitis

Skin dryness is usually the first sign of ICD and often starts in the web spaces between the fingers. This is referred to as the "sentinel sign".
What is irritant contact dermatitis?
Irritant contact dermatitis is the most common type of contact dermatitis. Usually irritant contact dermatitis builds up over time, and follows frequent, repeated exposure to skin irritants.
Skin dryness is usually the first sign of ICD and often starts in the web spaces between the fingers. This is referred to as the "sentinel sign". If the dryness persists, inflammation then develops, causing erythema and itch. The hands are the most common site for irritant contact dermatitis to occur.
Common irritants are:
- Water and wet work, for example frequent hand washing, prolonged glove use, dishwashing, food preparation, patient bathing in aged care and hospitals, and repeated client shampooing in hairdressing
- Soaps and detergents
- Cleaning agents
- Solvents such as turpentine, thinners and kerosene
- Oils and coolants
- Cement and other dusts
- Heat and sweating, especially if wearing occlusive gloves for extended periods of time
- Friction
People working in the following industries, especially those jobs which involve lots of ‘wet work’ and frequent contact with chemicals, are at highest risk. These include:
- Food handling
- Hair and beauty
- Healthcare
- Mechanical and metal working
- Construction
Good skin care is vital in the treatment and management of irritant contact dermatitis.
The likelihood of developing ICD is related to how irritating a particular substance is, plus the frequency and duration of exposure to this irritant. Once ICD has developed, it opens up the pathway for ACD to develop, increasing the risk of allergens entering the body via damage to the skin barrier.
Healing of the skin after an episode of ICD may take weeks or months, depending on the severity. If the dermatitis has been present for some time or if it has been severe, the skin may appear to have healed, but for several months there may be a lower threshold for developing dermatitis when exposed to skin irritants. ICD can be severe enough that people need job modification, or extended time away from work.
Wet work is one of the most common causes of irritant contact dermatitis. People often do not realise how many times a day their hands are wet or how many times a day they wash their hands. This is particularly the case for those working in the healthcare industry, or those with young children at home performing regular bathing, nappy changing, clothes washing and food preparation.
Allergic Contact Dermatitis
What is allergic contact dermatitis?
Allergic contact dermatitis (ACD) is a delayed type of allergy. ACD is an individual response in that a person may be allergic to something, that another person can use without problems.
It can occur at any time, even if someone has been using the same product for many years with no previous problems or just a few weeks. With this form of dermatitis, the rash appears 8 to 24 hours after skin contact and lasts for several days, and sometimes longer. It may develop after a spill, where there is prolonged exposure to a particular allergen, or with short, repeated exposures. ACD does not occur the first time an individual is exposed to a substance.
If the skin is already damaged from irritant contact dermatitis, the risk of becoming allergic to something is higher. This is because there is direct entry for the allergens to enter the body and cause allergy to develop. Once a contact allergy has developed, it tends to be life-long, and even the smallest amount of contact with that particular substance may cause the rash to appear again.
Not all chemicals cause allergy. Even if a substance causes allergy, not all people will become allergic to it. Only certain chemicals have the potential to cause allergic reactions. It is said that there are approximately 100,000 chemicals, but only about 5,000 have been reported to cause allergic contact dermatitis. Some very strong substances, such as kerosene, do not cause allergy, but are extremely irritating to the skin.
Whether people develop an allergic reaction depends on:
- The type of chemical contacted
- The molecular weight of a chemical; only chemicals with a small molecular weight will be able to penetrate the skin and initiate an allergic reaction
- The concentration of chemical on the skin
- The duration of skin contact
- The individual tendency to develop allergy
Common causes of contact allergy
- Fragrances used in skin cleansers and moisturisers
- Preservatives in skin care products such as methylisothiazolinone
- Nickel
- Chromate (found in cement and leather)
- Rubber chemicals (ingredients used in rubber gloves)
- Hair dye
- Glues and coatings e.g. epoxy resins
Sometimes causes of ACD are very specific to a particular occupation and/or workplace.

Contact Urticaria
What is contact urticaria?
Contact urticaria is a different type of allergy where the reaction starts shortly after contact with the allergen, usually within 10-30 minutes following skin contact. It is referred to as a Type 1 hypersensitivity. It normally settles down within an hour after contact with the causative allergen has stopped.
Recurrent episodes of contact urticaria can lead to dermatitis, termed protein contact dermatitis. This may technically appear just like allergic or irritant contact dermatitis.
Prick tests or blood tests measuring serum specific IgE are used to diagnose contact urticaria. At the SHI, prick testing is most commonly performed in food handlers who describe immediate symptoms or itching when handling a particular food such as fish or chicken. Prick testing for grasses, pollens or mould is not performed at the SHI. For this, referral to an allergist would be required.
Common causes are:
People with immediate allergy to substances like those listed above, may develop systemic symptoms such as asthma and usually they will need assessment by an allergist or immunologist.
- Natural rubber latex
- Hairdressing bleach (ammonium persulfate)
- Foods such as seafood, meat, chicken, wheat, rye and some fruit and vegetables
- House dust mite
- Malassezia furfur
Latex allergy
Latex allergy
Latex allergy is also a form of contact urticaria.
Healthcare workers (HCWs) are one of the occupational groups most affected by latex allergy from the use of latex gloves. Powdered disposable latex gloves increases the risk of latex allergy. The powder facilitates the transfer of the latex allergen to the skin and also aerosolises it, so latex proteins attached to the powder can be inhaled, ingested or enter the body via cracks and splits in the skin.
Some people with latex allergy can also be allergic to some fruits which have similar proteins to latex, including banana, avocado, kiwi fruit and melon.
People with immediate allergy to substances like latex, hairdressing bleach, wheat and rye may develop systemic symptoms such as asthma. Usually, they need assessment by an allergist or an immunologist.
Signs and symptoms of latex allergy
- An itchy, red rash within minutes of contacting latex
- Hives or welts on the skin
- Runny nose, sneezing and sometimes asthma
- Itchy eyes
- Burning, stinging, itching, tingling and swelling from latex contact on mucous membranes lining internal surfaces, like the mouth (from blowing up balloons or gloves worn by dentists), or the genitals (from condoms)
- Rarely, abdominal discomfort from ingestion of latex

Replace with supporting image
Testing for latex allergy and products that may contain latex
The symptoms normally resolve within an hour or two after contact has ceased.
Tests used to diagnose contact urticaria include blood tests and a different form of allergy testing, called prick testing. Prick testing is commonly used by allergists to diagnose causes of asthma, hay fever and food allergies. Prick testing involves lightly pricking the skin with a lancet which carries a tiny amount of a selected allergen into the body. The skin that was pricked is observed, watching for a red, itchy spot or hive, which usually occurs within minutes of the skin being pricked.
Serum specific IgE blood tests (formerly called radio-allergo-sorbent test or RAST tests) can also be used to diagnose latex allergy and are the safest option if severe latex allergy is suspected.
When testing for latex allergy, it is important that the phlebotomist or nurse performing this blood test does not wear latex gloves.
Patch testing is not used to diagnose latex allergy.
In addition to latex gloves causing latex allergy, there are many other medical and household products that may contain latex including:
- Reusable rubber gloves
- Rubber bands
- Rubber goggles
- Rubber innersoles
- Condoms
- Some computer mouse pads
- Panty hose or elastic in underwear
- Rubber electrical cords on appliances
- Rubber boots or raincoats
- Items with rubber handles such as toothbrushes, golf clubs, tennis racquets
- Medical products such as airway masks, catheters and dressings.
Patch testing is used to diagnose ACD.
Diagnosing ACD can be challenging. There is often a delay between exposure to the allergen and the development of dermatitis, which can make it difficult to link the exposure to the rash. People are often exposed to multiple allergens, particularly in the workplace. It is necessary for the clinician to have thorough knowledge of the many potential sources of allergens found in both workplaces and in recreational or domestic exposures.
Special note: In 2012, an allergen called methylisothiazolinone (MI) which is a preservative, was found to be causing very high rates of ACD. MI was found in cosmetics, sunscreens, baby wipes, make-up wipes, shampoo, conditioner, hair products, moisturisers, hand wash, shower gels and house paints. MI has been removed from most products, particularly baby wipes and sunscreens, but still found in some of the items listed above. It is very important to avoid this ingredient by reading ingredient lists and labels on all products used. It is now standard practice at the Skin Health Institute to advise all patients referred to the patch testing clinics to avoid MI prior to their appointment.
ICD is an important diagnosis for which there is no test available and often the diagnosis relies on the exclusion of allergic contact dermatitis (ACD) by patch testing.

Special note: In 2012, an allergen called methylisothiazolinone (MI) which is a preservative, was found to be causing very high rates of ACD. MI was found in cosmetics, sunscreens, baby wipes, make-up wipes, shampoo, conditioner, hair products, moisturisers, hand wash, shower gels and house paints. MI has been removed from most products, particularly baby wipes and sunscreens, but still found in some of the items listed above. It is very important to avoid this ingredient by reading ingredient lists and labels on all products used. It is now standard practice at the Skin Health Institute to advise all patients referred to the patch testing clinics to avoid MI prior to their appointment.